For Ebola virus disease, it came down to stopping the tradition of direct contact with the body of those who have died and dircet contact in general. For MERS it

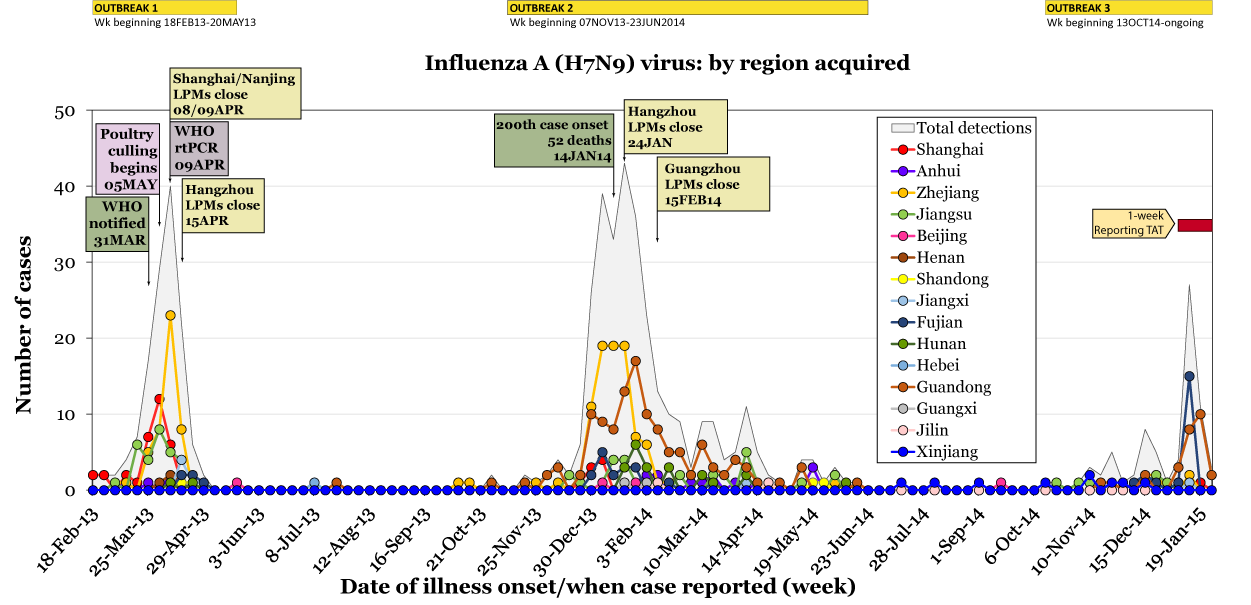
For influenza A(H7N9) virus cases, it is the habit of obtaining live poultry from retail markets where rare virus-laden chooks are culled and handed over because of a desire to see, choose and purchase the tastiest fresh chicken.
There is a common thread among these stories about direct contact or inefficiently droplet-transmitting virus infections: we can stop their spread.
But we also amplify and prolong their spread.
However, when it comes to human-adapted, efficient droplet-spread or airborne-transmitted viruses - well, then we're in trouble. Of course we could all just lock ourselves in a room for a few weeks but that won't ever happen.
So its very important to head off these "emerging" viruses while we still have a modicum of control over them. Once they get away from that control, and theoretically that could happen in the blink of an eye-right now even-no amount of fancy infra red cameras, poorly donned surgical masks or fancy hospitals laden with machines that blink and go ping, will stop them from spreading globally.
Cheery.
In the meantime - here's hoping China speeds up the closure of those live poultry markets. Habits can be changed but death is forever.
 |
| Click on image to enlarge. |


